Review of Back and Spine Anatomy and Kinesiology lecture notes.
Please click the link above and scan through the notes to review the basic anatomy and Kinesiology of the back and spine.
——
CONDITIONS OF THE BACK AND SPINE
Cervical Sprain/ Cervical Strain
– most commonly encountered cervical disorders
– has no neurological dysfunction
– radiographs are usually normal except for straightening of cervical lordosis secondary to muscle guarding
– condition is self-limiting
Cervical Sprain
– over stretching or tearing of ligaments or tendons, or both, secondary trauma
– superficial mms. are not tender upon palpation, but pain and neck stiffness are present
Cervical strain
– injury to muscles
– palpation shows tenderness of superficial muscles
———————————
Whiplash Injury

- most frequent cause of cervical sprain and strain
- 1/3 develops neck pain within 24 hrs. of injury
- most common mechanism: hyperextension injury to cervical spine from a rear-end motor vehicle collision
- May also have associated TMJ injuries
S et Sx
- neck pain and head aches
- neck fatigue, stiffness, pain with movement
- dizziness, lightheadedness, difficulty with concentration and memory
- PE shows: LOM of neck, (×) Spurling’s and Lhermitte’s, tenderness in anterior posterior neck structures, may have facet joint tenderness
—–
- Check for kerning-brudzinski sign – for meninigitis
——————————–
CERVICAL DISORDERS
3 General Types of Cervical disc disorders
- Internal disc disruption
– have pathological changes in the internal structure of the disc. - Degenerative disc disease
– have tears beginning in annulus and later progress, loss of disc height with annular bulging, loss of proteoglycans and water - Herniated nucleus pulposus
– occurs through weakening of the posterolateral annulus from repetitive stress
Manifestation:
discogenic pain
– usually vague and diffuse with axial distribution
– pain extending to arm usually on non dermatomal pattern
– symptoms intensified by coughing, Valsava and other activities that increase intradiscal pressure
radicular pain
– is deep dull and achy, or sharp, burning and electric in quality (depending on type of involvement: primary motor or dorsal root)
——————————————————
CERVICAL SPONDYLOSIS (OSTEOARTHRITIS)
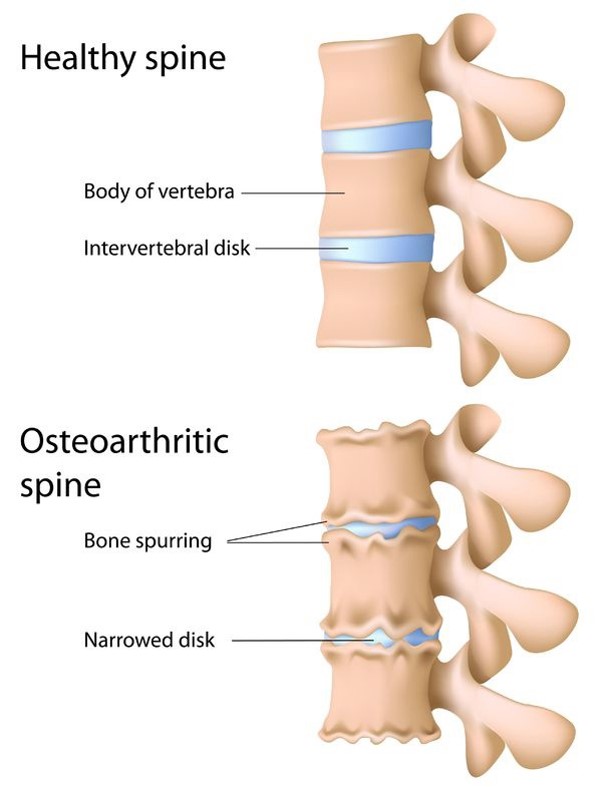
Spondylosis – describes the degenerative changes that occur in the intervertebral discs and vertebral bodies
Osteoarthritis (OA)- involve degenerative changes in the zygapophyseal and uncovertebral joints
Factors the contribute to the degenerative changes of the vertebral spine: Aging, trauma, work activities and genetics
—————————————————-
Torticollis (Wryneck)
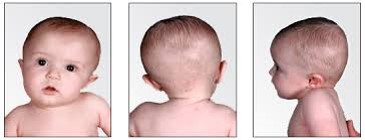
- deformity of the neck which includes elements of both rotation and of flexion
- usually, one sternocleidomastoid muscle is shortened which results to tilting of the head toward the affected side and rotation of the chin to the opposite side.
- Maybe congenital or acquired
————————-
Thoracic Outlet Syndrome
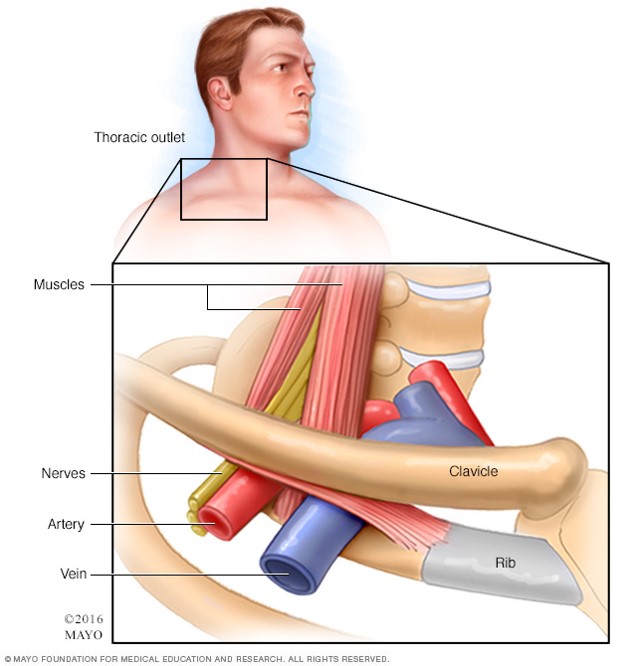
- compression of the subclavian artery
- by a bony abnormality such as a cervical rib (cervical rib syndrome)
————————–
AFFECTIONS OF THE SPINE AND THORAX
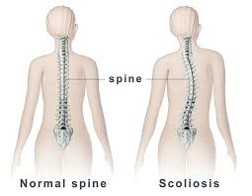
- lateral curvature of the spine

Measurement of Curvature
- Cobb method- developed by John R. Cobb
- Risser-Fergusson method
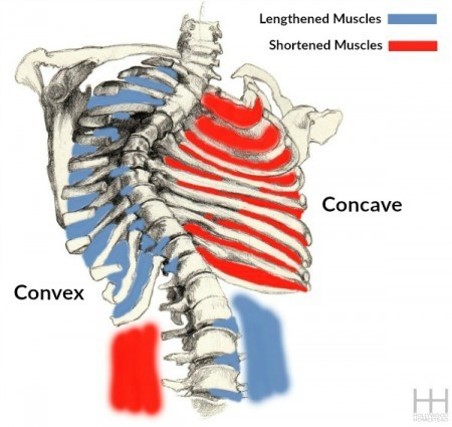
Long C-Curve - extends the length of the thoracic and lumbar spines
- often uncompensated: higher shoulder on the convex side high pelvis on the concave side
S Curve - most common type of curve seen in idiopathic scoliosis: R thoracic, L lumbar
- involves a major curve and a compensatory curve
- usually associated with structural changes on the major curve
Mild scoliosis
– curves less than 20 degrees
– curves less than 10 degrees are considered normal and do not need tx
Moderate Scoliosis
– curves from 20 to 40 or 50 degrees
– associated with early structural changes in the vertebrae and rib cage
Severe Scoliosis
– Curves of 40 to 50 degrees or greater
– Curves with 60 to 70 degrees or greater are associated with significant cardiopulmonary
Changes and decreased life expectancy
– <55 deg- no changes in pulmonary function
– >55 deg- progressive loss of pulmonary function
– 100 deg- patient becomes symptomatic
– >100 deg- lead to pulmonary disability
———————-
Kyphosis / Lordosis
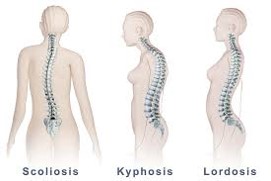
Kyphosis
– anteroposterior curvature of the spine in which the convexity is directed posteriorly ´most frequent cause is faulty posture
Adolescent Kyphosis (Scheuermann’s Dis., Juvenile Kyphosis, Vertebral epiphysitis)
– chronic affection of the vertebral bodies evidenced clinically by the gradual development of a fixed kyphosis with or without back pain
Lordosis
– anteroposterior curvature of the spine in which the concavity is directed posteriorly
´2 common causes:
1. abnormal dorsal kyphosis – a compensatory in lumbar lordosis is necessary for patient to stand upright
2. flexion contracture – in lumbar lordosis is necessary to tilt the pelvis in order to stand erect
—————–
Low Back Pain
Types of Low Back Pain:
Static LBP
– Excessive lordosis or “sway back” posture is responsible for 75% of all static or postural LBP which is usually seen in:
a. pregnant women who stand with an arched back
b. improper sitting position
c. persons wearing high-heeled shoes
d. people with poor sleeping habits (prone)
e. prolonged sitting and standing
Kinetic LBP
– implies irritation of pain-sensitive tissues activated by movement of the spine
The following are Pain-free structures:
– IV disk (nucleus pulposus, inner and middle layer of annulus fibrosus)
– Veretbral Body
The ff structures are Pain Sensitive:
– Outer layers of annulus fibrosus
– Nerve root
– Anterior longitudinal ligament
– Posterior longitudinal ligament
– Erector spinae
– Recurrent nerve of the nerve root
– Zygapophyseal joints –
– other posterior supporting ligaments
——————–
Abnormalities of the Bony Structure of the Low Back

Spondylolisthesis
– forward slipping of a vertebra forward slipping of a vertebra and the superincumbent spinal column on the vertebra below
– occurs most commonly: L5 on S1 and L4 over L5
-graded according to displacement:
25%
26-50%
51-75%
>75%
Spondylosis
– degenerative changes in the spine
– stiffness is the main feature
– pain may radiate to the buttocks
– dull and nugging pain & stiffness in the morning
– treated by bedrest
– use of hydrotherapy is said to be beneficial
Spondylolysis- fracture of the pars interarticularis (part of the pedicle)
– commonly becomes bilateral that leads to spondylolisthesis
– commonly involving L5 vertebrae & occasionally, L4
– incidence: M>F
– S/Sx: localized lumbosacral pain that is usually worst with extension and partially relieved with flexion
Spinal Stenosis
– localized narrowing of spinal canal from a structural abnormality of its bony components
– greatest central canal narrowing occurs at L3-L4 and L4-L5 regions
————
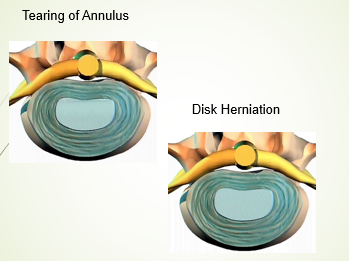
Herniated Disks
– NP protrudes out from between the vertebrae
– nerves are impinged by the bulging NP
– lead to numbness and/or pain
___________
Ankylosing Spondylitis
-is a type of arthritis that affects the spine.
-symptoms include pain and stiffness from the neck down to the lower back.
– The spine’s bones (vertebrae) fuse together, resulting in a rigid spine.
– These changes may be mild or severe, and may lead to a stooped-over posture.
-AKA Bamboo Spine
